Childhood Apraxia of Speech (CAS) is a motor speech disorder. CAS is a relatively uncommon disorder (1-2 children per 1,000= 0.1-0.2%) and one of the lesser known disorders treated by Speech-Language Pathologists. There are some identified causes of CAS (e.g., stroke, trauma, chromosomal abnormalities) but we are not truly sure of all of the causes.
In a nutshell:
The child knows what he/she wants to say and the brain sends the message to the mouth (lips, jaw, and tongue) for appropriate placement to produce sounds, but the mouth doesn't cooperate.
In a nutshell:
The child knows what he/she wants to say and the brain sends the message to the mouth (lips, jaw, and tongue) for appropriate placement to produce sounds, but the mouth doesn't cooperate.
Keep Reading for information on Symptoms, Testing, Diagnosis, Treatment, and Resources
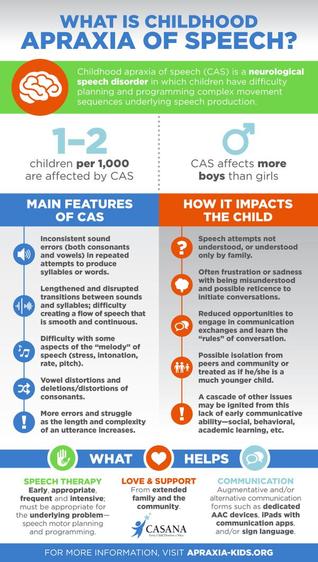
Signs/Symptoms:
- Inconsistent misarticulation errors
- Vowel distortions/omissions/substitutions
- Limited consonants used (frequently only b and d)
- Oral “groping” behaviors- moving their mouth but nothing is coming out (Not all children exhibit this at all times or situations. If your child does not demonstrate groping of their speech musculature, that alone is not enough to rule out CAS.)
- Odd prosody (intonation)/ monotone speech (commonly termed: robotic speech)
- More errors with increasing complexity
- Limited or no babbling as an infant
- High frequency words (e.g. hi, bye, mom) can be clearly articulated
- Says something clearly one time and doesn’t say it again
- Cannot correct misproductions solely with modeling/imitation
Testing and Diagnosis:
Identification and treatment are vital to each child's future communicative success. Testing and diagnosis of Childhood Apraxia of Speech (CAS) is provided by a Speech-Language Pathologist (SLP). SLPs rely on parental input, observations of the child’s verbal productions and behaviors, informal testing (speech sample analysis), and formal tests like the Kaufman Speech Praxis Test in order to identify CAS. Testing and identification may be done as easy at 2 years of age; however, firm diagnosis may be difficult to establish until the child is able to fully participate in the tasks required by the SLP who is evaluating them. Equally important is that the SLP understands appropriate diagnosis techniques and the core characteristics that differentiate CAS from other types of speech problems. Regardless, the disorder can be “suspected” and early help can and should begin. Often, a few months of “diagnostic therapy” can help to determine if CAS is the main issue that is causing a child to have difficulty speaking.
Treatment:
Treatment for CAS differs from traditional articulation and phonological treatments. ABA treatment strategies are counterproductive, as well, and can often times magnify symptoms. When non-CAS treatments are implemented with a child with CAS the results commonly are increased frustration, refusal to talk/engage, and lack of progress in therapy. At times, an Augmentative Communication Device (AAC) is utilized in order to assist in communication tasks and to provide stress-free modeling for the child. CAS should ONLY be treated by (or under the close advisement of) a licensed Speech-Language Pathologist.
Important things to remember:
People with CAS oftentimes do NOT have cognitive impairments (they understand fully).
People with CAS do NOT need you to speak loudly or slowly.
People with CAS know what they want to say.
People with CAS don’t need you to “pretend” you understand them.
People with CAS do NOT need you to try to complete their sentences.
When frustrated (or to avoid frustration), people with CAS respond well to Yes/No questions.
If you have concerns that your child may have Childhood Apraxia of Speech (CAS) talk to your pediatrician, speech-language pathologist, or give us a call!
Resources:
https://www.apraxia-kids.org/
https://www.asha.org/


 RSS Feed
RSS Feed